Heart Failure Survival Prediction Using Machine Learning
Project Background:
Cardiovascular disease is still an important cause of morbidity and mortality worldwide. Heart failure, which is an inability for the heart to pump blood efficiency, can be fatal and diagnosis challenging. While traditional machine learning has not been extensively used in clinical medicine outside of academic research environments, there are many different applications of this.
Heart failure can be particularly devastating and caused by a wide variety of different clinical entities. Many times, the cause is unknown. Certain therapies have been shown to improve outcomes in heart failure, but is there a way to better detect mortality from heart failure to perhaps increase monitoring and improve management of heart failure patients?
Dataset Description:
This project focuses on a dataset that was used in the medical journal of BMC Medical Informatics and Decision Making. The citation of the dataset and the research article is publicly available by PLOS.
The dataset can be found at the following URL:
The target variable in the dataset is classified as Event with a value of 1 signifying death in the study. All subjects in this study were diagnosed with heart failure. There were otherwise 12 other features to use in the prediction of death including age, gender, smoking status, diabetes, anemia, ejection fraction, sodium level, creatinine, CPK, and platelets.
Reference Cited:
Chicco, D., & Jurman, G. (2020). Machine learning can predict survival of patients with heart failure from serum creatinine and ejection fraction alone. BMC Medical Informatics and Decision Making, 20(1). doi:10.1186/s12911-020-1023-5
Data Cleaning, Exploration, and Analysis
The data was loaded into Python and cleaned for further exploratory data analysis. Columns were renamed and Python was queried for any null values, of which there were none.
| Time | Event | Gender | Smoking | Diabetes | BP | Anemia | Age | EF | Sodium | Creatinine | Platelets | CPK | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 | 97 | 0 | 0 | 0 | 0 | 0 | 1 | 43.0 | 50 | 135 | 1.30 | 237000.00 | 358 |
| 1 | 180 | 0 | 1 | 1 | 1 | 0 | 1 | 73.0 | 30 | 142 | 1.18 | 160000.00 | 231 |
| 2 | 31 | 1 | 1 | 1 | 0 | 1 | 0 | 70.0 | 20 | 134 | 1.83 | 263358.03 | 582 |
| 3 | 87 | 0 | 1 | 0 | 0 | 0 | 1 | 65.0 | 25 | 141 | 1.10 | 298000.00 | 305 |
| 4 | 113 | 0 | 1 | 0 | 0 | 0 | 0 | 64.0 | 60 | 137 | 1.00 | 242000.00 | 1610 |
| ... | ... | ... | ... | ... | ... | ... | ... | ... | ... | ... | ... | ... | ... |
| 294 | 250 | 0 | 0 | 0 | 1 | 0 | 0 | 45.0 | 55 | 132 | 1.00 | 543000.00 | 582 |
| 295 | 244 | 0 | 0 | 0 | 1 | 0 | 0 | 51.0 | 40 | 134 | 0.90 | 221000.00 | 582 |
| 296 | 14 | 1 | 1 | 0 | 0 | 0 | 0 | 45.0 | 14 | 127 | 0.80 | 166000.00 | 582 |
| 297 | 80 | 0 | 1 | 0 | 1 | 0 | 0 | 60.0 | 45 | 133 | 1.00 | 297000.00 | 897 |
| 298 | 16 | 0 | 0 | 0 | 0 | 1 | 1 | 65.0 | 25 | 137 | 1.30 | 276000.00 | 52 |
299 rows × 13 columns
Description of the Variables
The variables and data types are listed below. The variables were coded into Python to account for categorical values.
TIME: Integer, signifying length of follow-up in days.
Event: Categorical (0: Died, 1: Alive)
Gender: Categorical (0: Female, 1: Male)
Smoking: Categorical (0: Non-Smoker, 1: Smoker)
Diabetes: Categorical (0: No Diabetes, 1: Diabetes)
BP: Categorical (0: No Hypertension, 1: Has Hypertension)
Anaemia: Categorical (0: No Anemia, 1: Anemia)
Age: Float (in years)
Ejection.Fraction: Integer (percentage)
Sodium: Integer (mg/dL)
Creatinine: Float (mg/dL)
Platelets: Float (mg/dL)
CPK: Integer
A descriptive analysis was performed on the numerical variables as well as the target variable.
Description of Numerical Categories
| Time | Age | EF | Sodium | Creatinine | Platelets | CPK | |
|---|---|---|---|---|---|---|---|
| count | 299.000000 | 299.000000 | 299.000000 | 299.000000 | 299.00000 | 299.000000 | 299.000000 |
| mean | 130.260870 | 60.833893 | 38.083612 | 136.625418 | 1.39388 | 263358.029264 | 581.839465 |
| std | 77.614208 | 11.894809 | 11.834841 | 4.412477 | 1.03451 | 97804.236869 | 970.287881 |
| min | 4.000000 | 40.000000 | 14.000000 | 113.000000 | 0.50000 | 25100.000000 | 23.000000 |
| 25% | 73.000000 | 51.000000 | 30.000000 | 134.000000 | 0.90000 | 212500.000000 | 116.500000 |
| 50% | 115.000000 | 60.000000 | 38.000000 | 137.000000 | 1.10000 | 262000.000000 | 250.000000 |
| 75% | 203.000000 | 70.000000 | 45.000000 | 140.000000 | 1.40000 | 303500.000000 | 582.000000 |
| max | 285.000000 | 95.000000 | 80.000000 | 148.000000 | 9.40000 | 850000.000000 | 7861.000000 |
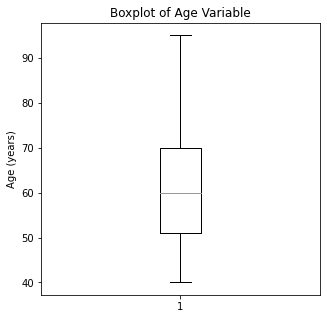
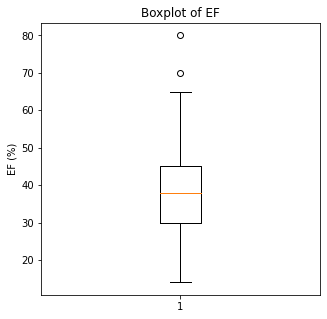
The numerical variables have some interesting descriptive statistics. The lowest age was 40 and the oldest person was 95. The lowest ejection fraction was 14% and the maximum was 80%. There was a significantly low sodium value of 113 and a high level of 148. For reference, normal sodium levels are between 135-145. The highest creatinine was 9.4 which is exceedingly high. Likewise, the lowest platelet value was 25K and the highest was 850000. CPK, a muscle enzyme, had minimums of 23K with maximum of 7800K.
Looking at the means, the mean follow-up time was 130 days, age 60, EF of 38%, sodium of 136, creatinine of 1.39 (slightly elevated), 263K platelets (which is normal), and CPK of 481.
Description of Categorical Variables
| Event | Gender | Smoking | Diabetes | BP | Anemia | |
|---|---|---|---|---|---|---|
| count | 299 | 299 | 299 | 299 | 299 | 299 |
| unique | 2 | 2 | 2 | 2 | 2 | 2 |
| top | 0 | 1 | 0 | 0 | 0 | 0 |
| freq | 203 | 194 | 203 | 174 | 194 | 170 |
Based on the categorical variables, more patients were alive, male, non-smokers, non-diabetic, non-anemic, and with normal blood pressure.
To eliminate redundant variables, a correlation analysis and a correlation plot was generated to identify correlations with an absolute value of >0.95.
| Time | Age | EF | Sodium | Creatinine | Platelets | CPK | |
|---|---|---|---|---|---|---|---|
| Time | 1.000000 | -0.224068 | 0.041729 | 0.087640 | -0.149315 | 0.010514 | -0.009346 |
| Age | -0.224068 | 1.000000 | 0.060098 | -0.045966 | 0.159187 | -0.052354 | -0.081584 |
| EF | 0.041729 | 0.060098 | 1.000000 | 0.175902 | -0.011302 | 0.072177 | -0.044080 |
| Sodium | 0.087640 | -0.045966 | 0.175902 | 1.000000 | -0.189095 | 0.062125 | 0.059550 |
| Creatinine | -0.149315 | 0.159187 | -0.011302 | -0.189095 | 1.000000 | -0.041198 | -0.016408 |
| Platelets | 0.010514 | -0.052354 | 0.072177 | 0.062125 | -0.041198 | 1.000000 | 0.024463 |
| CPK | -0.009346 | -0.081584 | -0.044080 | 0.059550 | -0.016408 | 0.024463 | 1.000000 |
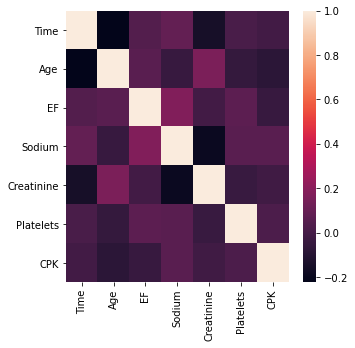
Based on the numerical values as well as the correlation map, there do not appear to be any highly correlated variables.
The distribution of the variables was then visualized after splitting up the numerical and categorical data.
#Visualizing Numerical Data
#Setting Figure Size
plt.figure(figsize=[100,100])
f,a = plt.subplots(4,2, figsize=(60,30))
a = a.ravel()
for idx, ax in enumerate(a):
ax.hist(df_num.iloc[:,idx], bins = 150)
ax.set_title(df_num.columns[idx], size = 40)
ax.set_ylabel('Counts', size = 20)
plt.show()
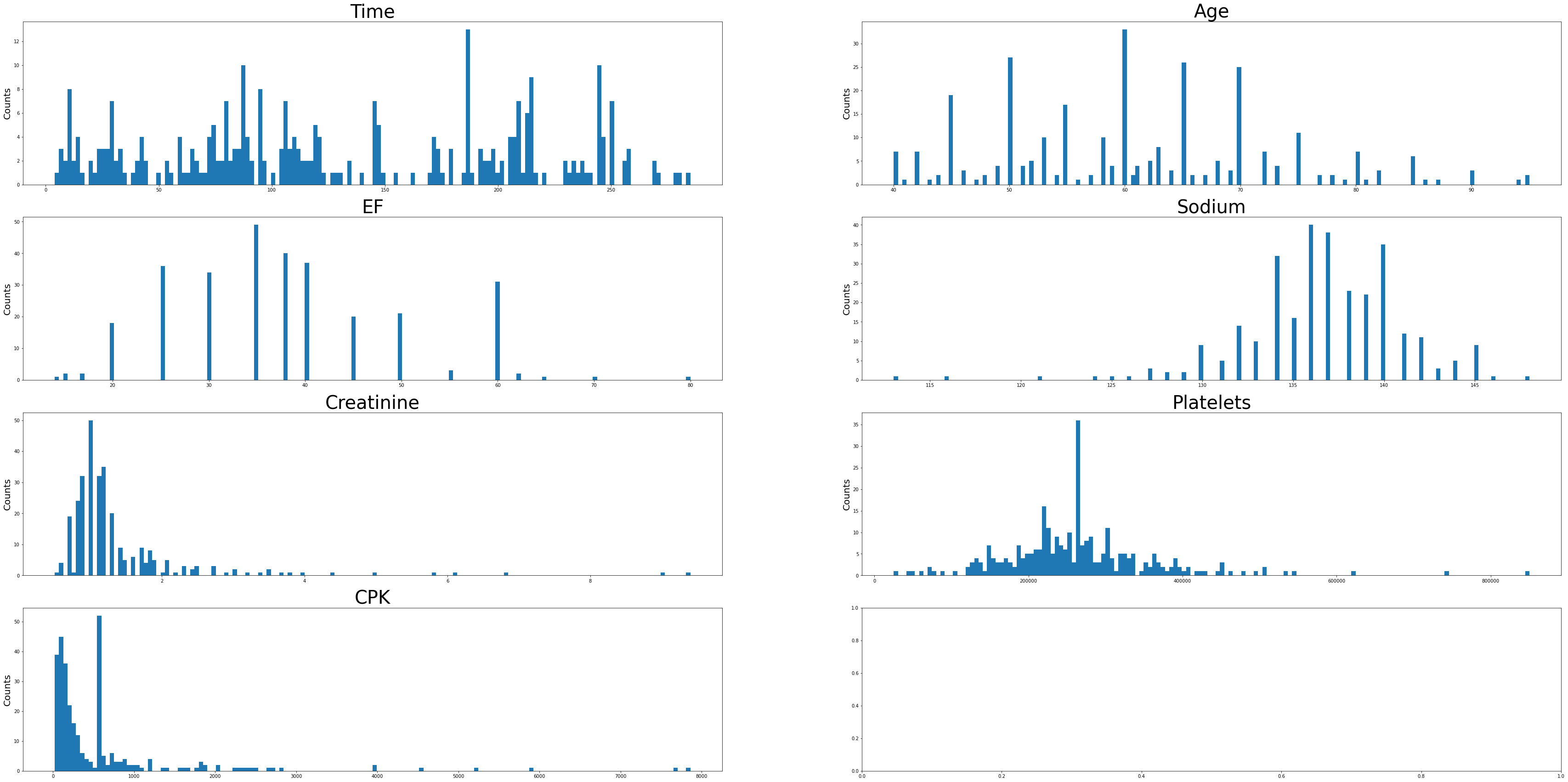
Sodium levels have positive skew, while creatinine, platelets, EF, and CPK levels appear negatively skewed. The Time variable has a multimodal distribution. Age looks to be approximately normally distributed with a slight positive skew.
The categorical variables were then analyzed.
#Visualizing Categorical Data
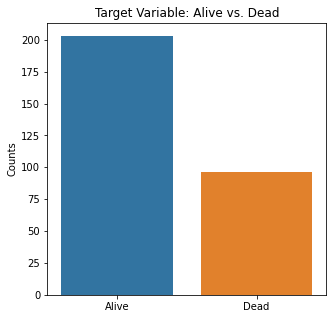
sns.countplot(x = 'Event', data = df_cat)
plt.title('Target Variable: Alive vs. Dead')
plt.xticks([0,1], ['Alive', 'Dead'])
plt.xlabel(xlabel = None)
plt.ylabel('Counts')
plt.show()
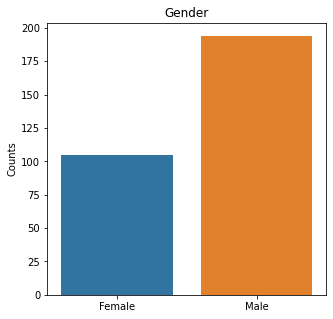
sns.countplot(x = 'Gender', data = df_cat)
plt.title('Gender')
plt.xticks([0,1], ['Female', 'Male'])
plt.xlabel(xlabel=None)
plt.ylabel('Counts')
plt.show()
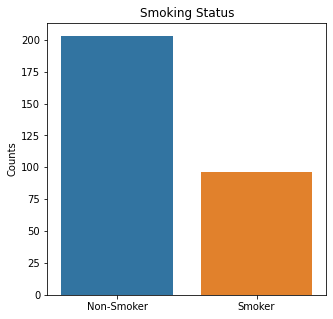
sns.countplot(x = 'Smoking', data = df_cat)
plt.title('Smoking Status')
plt.xticks([0,1], ['Non-Smoker', 'Smoker'])
plt.xlabel(xlabel=None)
plt.ylabel('Counts')
plt.show()
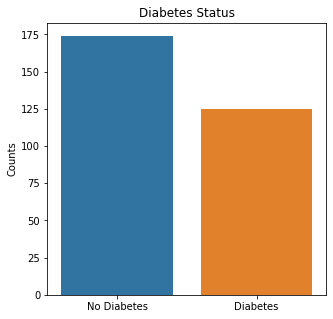
sns.countplot(x = 'Diabetes', data = df_cat)
plt.title('Diabetes Status')
plt.xticks([0,1], ['No Diabetes', 'Diabetes'])
plt.xlabel(xlabel=None)
plt.ylabel('Counts')
plt.show()
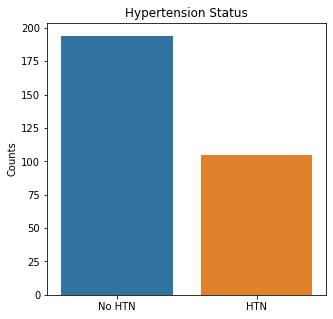
sns.countplot(x = 'BP', data = df_cat)
plt.title('Hypertension Status')
plt.xticks([0,1], ['No HTN', 'HTN'])
plt.xlabel(xlabel=None)
plt.ylabel('Counts')
plt.show()
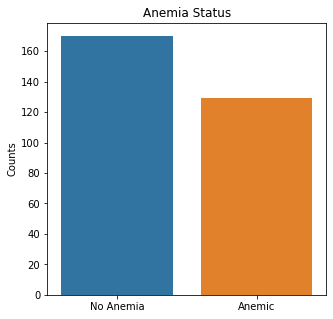
sns.countplot(x = 'Anemia', data = df_cat)
plt.title('Anemia Status')
plt.xticks([0,1], ['No Anemia', 'Anemic'])
plt.xlabel(xlabel=None)
plt.ylabel('Counts')
plt.show()
There were almost two times as many alive participants as dead participants in the study. The majority of the participants were males, non-smokers, non-diabetic, without high blood pressure, and were not anemic.
The numerical variables were then visualized using boxplots to visualize for outliers.
#Visualizing Boxplots to Assess for Outliers
plt.boxplot(df['Time'])
plt.title('Boxplot of Time Follow-Up Variable')
plt.ylabel('Time (Days)')
plt.show()
plt.boxplot(df['Age'])
plt.title('Boxplot of Age Variable')
plt.ylabel('Age (years)')
plt.show()
plt.boxplot(df['EF'])
plt.title('Boxplot of EF')
plt.ylabel('EF (%)')
plt.show()
plt.boxplot(df['Sodium'])
plt.title('Boxplot of Sodium Level')
plt.ylabel('Sodium (mg/dL)')
plt.show()
plt.boxplot(df['Creatinine'])
plt.title('Boxplot of Creatinine')
plt.ylabel('Creatinine (mg/dL)')
plt.show()
plt.boxplot(df['Platelets'])
plt.title('Boxplot of Platelets')
plt.ylabel('Platelets (mg/dL)')
plt.show()
plt.boxplot(df['CPK'])
plt.title('Boxplot of CPK Level')
plt.ylabel('CPK (mg/dL)')
plt.show()
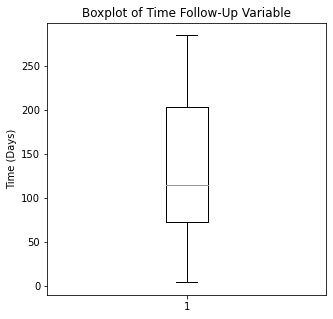
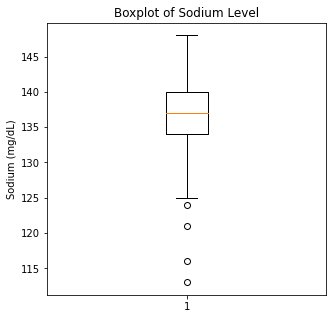
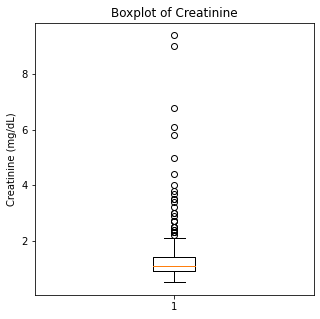
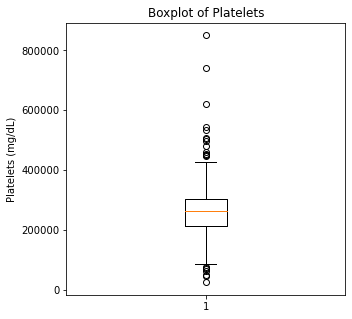
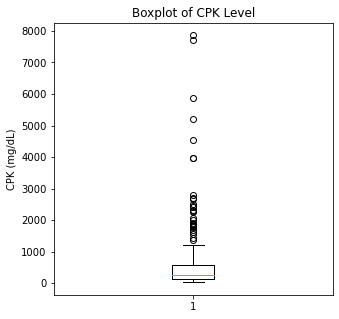
There are some significant outliers in these variables, specifically regarding creatinine levels, CPK, platelet levels, and to some extent sodium levels. We will keep these outliers in the dataset as these significant outliers could be predictive of worse prognosis and deleting them would affect our algorithms.
Using swarm plots, the numerical variables were plotted against the target variable of survival.
#Visualizing Swarm Plots to Compare The Target Variable to Our Explanatory Variables
categories = df.Event
sns.swarmplot(categories, df.Time)
plt.title('Survival vs. Follow-Up Time')
plt.xlabel(xlabel = None)
plt.ylabel('Follow-Up (Days)')
plt.xticks([0,1], ['Alive', 'Dead'])
plt.show()
sns.swarmplot(categories, df.Age)
plt.title('Survival vs. Age')
plt.xlabel(xlabel = None)
plt.ylabel('Age (years)')
plt.xticks([0,1], ['Alive', 'Dead'])
plt.show()
sns.swarmplot(categories, df.EF)
plt.title('Survival vs. Ejection Fraction')
plt.xlabel(xlabel = None)
plt.ylabel('Ejection Fraction (%)')
plt.xticks([0,1], ['Alive', 'Dead'])
plt.show()
sns.swarmplot(categories, df.Sodium)
plt.title('Survival vs. Sodium Level')
plt.xlabel(xlabel = None)
plt.ylabel('Sodium Level (mg/dL)')
plt.xticks([0,1], ['Alive', 'Dead'])
plt.show()
sns.swarmplot(categories, df.Creatinine)
plt.title('Survival vs. Creatinine Level')
plt.xlabel(xlabel = None)
plt.ylabel('Creatinine (mg/dL)')
plt.xticks([0,1], ['Alive', 'Dead'])
plt.show()
sns.swarmplot(categories, df.Platelets)
plt.title('Survival vs. Platelets Level')
plt.xlabel(xlabel = None)
plt.ylabel('Platelets (mg/dL)')
plt.xticks([0,1], ['Alive', 'Dead'])
plt.show()
sns.swarmplot(categories, df.CPK)
plt.title('Survival vs. CPK Level')
plt.xlabel(xlabel = None)
plt.ylabel('CPK (mg/dL)')
plt.xticks([0,1], ['Alive', 'Dead'])
plt.show()
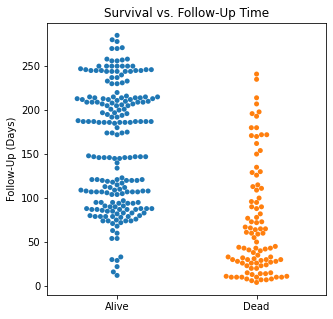
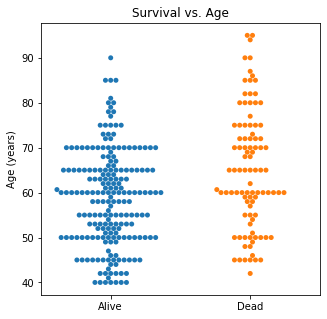
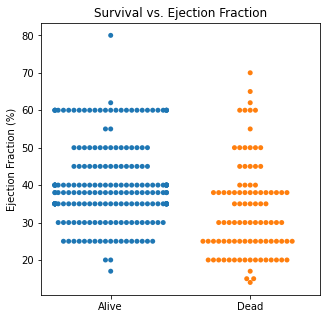
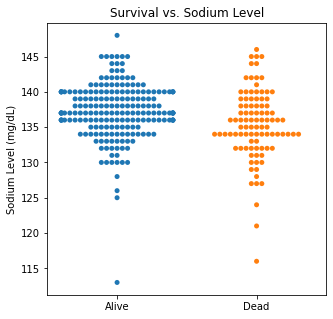
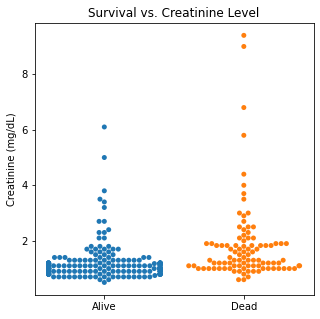
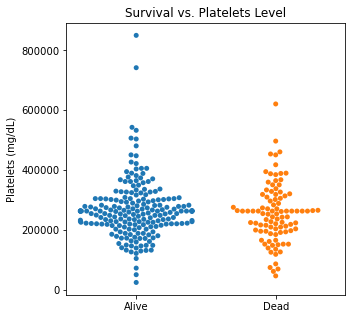
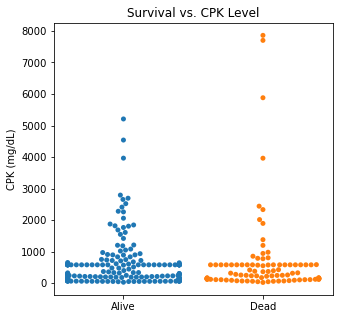
There are several interesting findings when plotting survival vs our different numerical variables. Unsurprisingly, those who had longer follow-up in days were more likely to be alive. There was a trend that the older individuals were more likely to not have survived. There appears to be an association between lower EF and survival and this is logical. However, looking at the distributions, there was not a significant difference between the two. Likewise, there did not seem to be a significant difference between sodium level and survival. The higher the level of creatinine above 2, the more likely they were not to survive. These creatinine levels are exceedingly high and the higher the creatinine, the higher the likelihood of kidney failure which explains this trend. There did not seem to be a significant difference between survival and the platelet/CPK levels.
Machine Learning Algorithms
In general, when fitting the data using various models, the false negatives or predicting survival when the patient could be at risk of death should be minimized if at all possible. The risk of predicting someone who is at higher risk of death who truly is not at risk would not be as catastrophic as a false negative. The algorithms were evaluated using precision, recall, F1 scores, and ROC curves. The machine learning algorithms that were used were Logistic Regression, K-Nearest Neighbors, Support Vector Machine, Random Forest, and XG Boost.
Logistic Regression
#Importing Packages
from sklearn.model_selection import train_test_split
from sklearn.linear_model import LogisticRegression
from sklearn.preprocessing import StandardScaler
from sklearn.metrics import classification
from yellowbrick.classifier import ConfusionMatrix, ClassificationReport, ROCAUC
#Creating Features and Target Objects
features = df.loc[:, df.columns != 'Event']
target = df['Event']
#Getting Dummies for Our Categoricals
features = pd.get_dummies(features)
#Creating Standardizer and Logit Objects
standardizer = StandardScaler()
logit = LogisticRegression()
#Standardizing Features
features_standardized = standardizer.fit_transform(features)
#Train/Test Split
features_train, features_test, target_train, target_test = train_test_split(features_standardized, target, test_size = 0.2)
#Fitting Data to Logistic Regression Classifier
logreg = logit.fit(features_train, target_train)
#Confusion Matrix Visualizer
classes = ['Survived', 'Not Survived']
cm = ConfusionMatrix(logit, classes = classes, percent = False)
#Fitting Passed Model
cm.fit(features_train, target_train)
cm.score(features_test, target_test)
#Changing Fontsize in Figure
for label in cm.ax.texts:
label.set_size(20)
cm.poof()
#Configuring Graph Parameters
plt.rcParams['figure.figsize'] = (15,7)
plt.rcParams['font.size'] = 20
visualizer = ClassificationReport(logit, classes = classes)
visualizer.fit(features_train, target_train)
visualizer.score(features_test, target_test)
g = visualizer.poof()
#ROC/AUC Curve
roc = ROCAUC(logit)
roc.fit(features_train, target_train)
roc.score(features_test, target_test)
g = roc.poof()
#Checking Variable Feature Importance
from yellowbrick.model_selection import FeatureImportances
#Getting Labels and Checking Feature Importance for Log Reg Model
labels = list(map(lambda x: x.title(), features))
viz = FeatureImportances(logreg, labels = labels)
viz.fit(features_train, features_test)
viz.show()
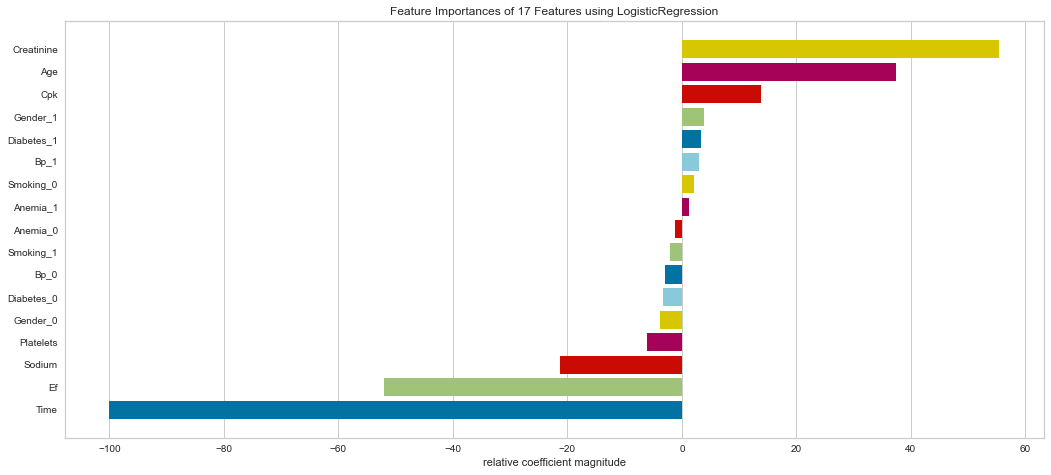
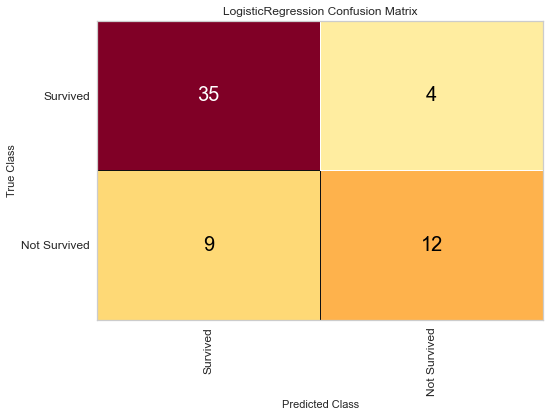
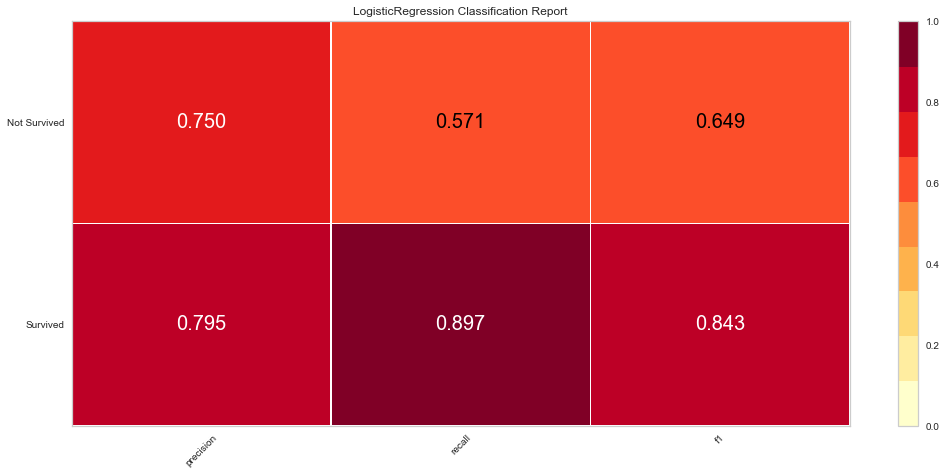
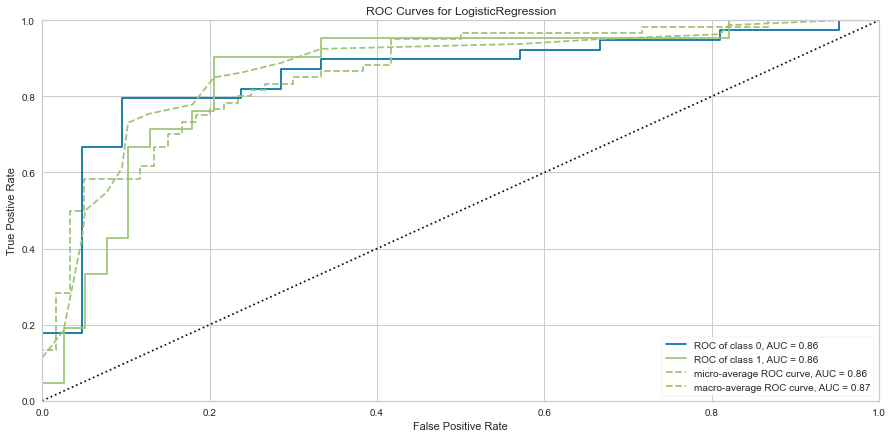
The logistic regression model performed reasonably well with an F1 score of 0.615 of predicting death and 0.815 of predicting death. There were 9 false negatives in this model. The ROC was 0.81 for both class predictions. After checking feature importance based on the logistic regression model, age, creatinine, CPK levels, and female gender were some of the most important features based on relative coefficients.
KNN
#Importing Packages
from sklearn.neighbors import KNeighborsClassifier
from sklearn.model_selection import GridSearchCV, RandomizedSearchCV
from sklearn.metrics import classification_report, confusion_matrix
#Getting Dummies for Target Variable
target = pd.get_dummies(df['Event'])
#Train/Test 80/20 Split
features_train, features_test, target_train, target_test = train_test_split(features_standardized, target, test_size = 0.2, random_state = 1)
#Starting with KNN of 3
knn = KNeighborsClassifier(n_neighbors = 3, n_jobs = -1)
knn.fit(features_train, target_train)
#Visualizing Metrics
target_pred = knn.predict(features_test)
test = np.array(target_test).argmax(axis=1)
predictions = np.array(target_pred).argmax(axis=1)
print('Confusion Matrix:\n', confusion_matrix(test, predictions), '\n')
print('Classification Report:\n', classification_report(test, predictions), '\n')
Confusion Matrix:
[[34 7]
[11 8]]
Classification Report:
precision recall f1-score support
0 0.76 0.83 0.79 41
1 0.53 0.42 0.47 19
accuracy 0.70 60
macro avg 0.64 0.63 0.63 60
weighted avg 0.69 0.70 0.69 60
The optimized hyperparameters for KNN were a leaf size of 1, p of 2, n_neighbors of 5, uniform weights, and the Minkowski metric. The model was re-run with the tuned model.
Confusion Matrix:
[[36 5]
[13 6]]
Classification Report:
precision recall f1-score support
0 0.73 0.88 0.80 41
1 0.55 0.32 0.40 19
accuracy 0.70 60
macro avg 0.64 0.60 0.60 60
weighted avg 0.67 0.70 0.67 60
Interestingly, using hyperparameter tuning this model had better success at predicting death than survival. However, there were 13 false negatives which we would want to avoid. The F1 scores are not as high as the logistic regression model unfortunately.
Support Vector Machine Classifier
#Importing Packages
from sklearn.svm import SVC
#Resetting our Target Object to Not Have Dummy Variables
target = df['Event']
#Creating SVM Object
svc = SVC(kernel='linear')
#Train/Test 80/20 Split
features_train, features_test, target_train, target_test = train_test_split(features_standardized, target, test_size = 0.2, random_state = 1)
svc.fit(features_train, target_train)
cm_svc = ConfusionMatrix(svc, classes = classes, percent = False)
cm_svc.fit(features_train, target_train)
cm_svc.score(features_test, target_test)
cm_svc.poof()
svc_vis = ClassificationReport(svc, classes = classes)
svc_vis.fit(features_train, target_train)
svc_vis.score(features_test, target_test)
svc_vis.poof()
svc_roc = ROCAUC(svc, micro = False, macro = False, per_class = False)
svc_roc.fit(features_train, target_train)
svc_roc.score(features_test, target_test)
svc_roc.poof()
#Checking Feature Importance
labels = list(map(lambda x: x.title(), features))
viz = FeatureImportances(svc, labels = labels)
viz.fit(features_train, features_test)
viz.show()
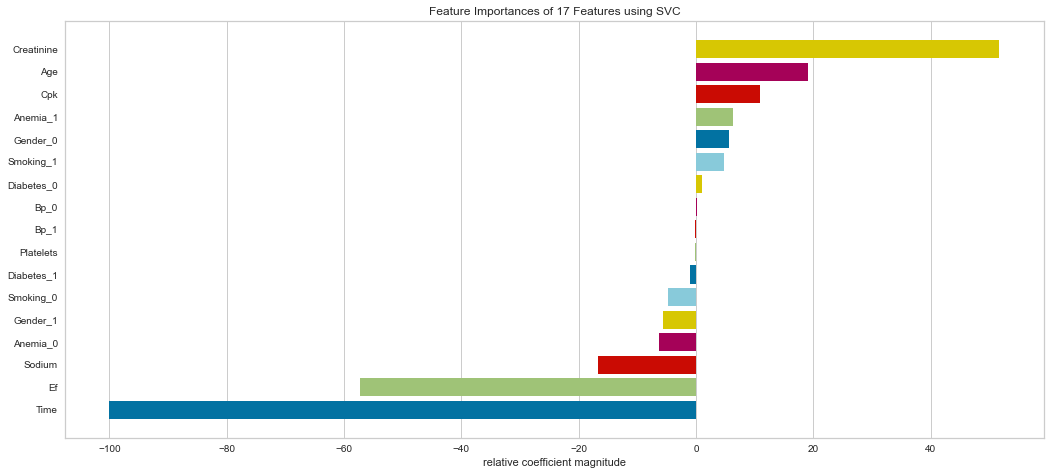
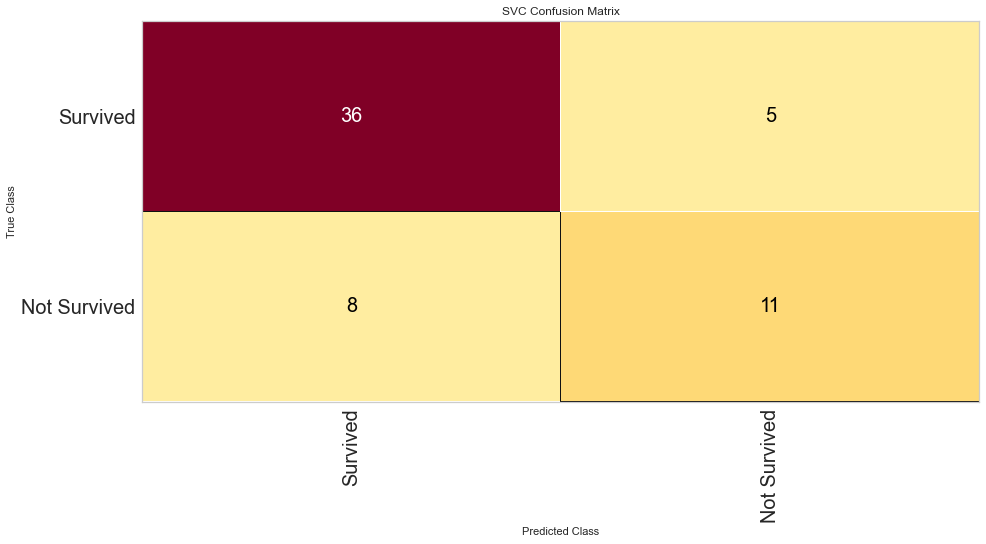
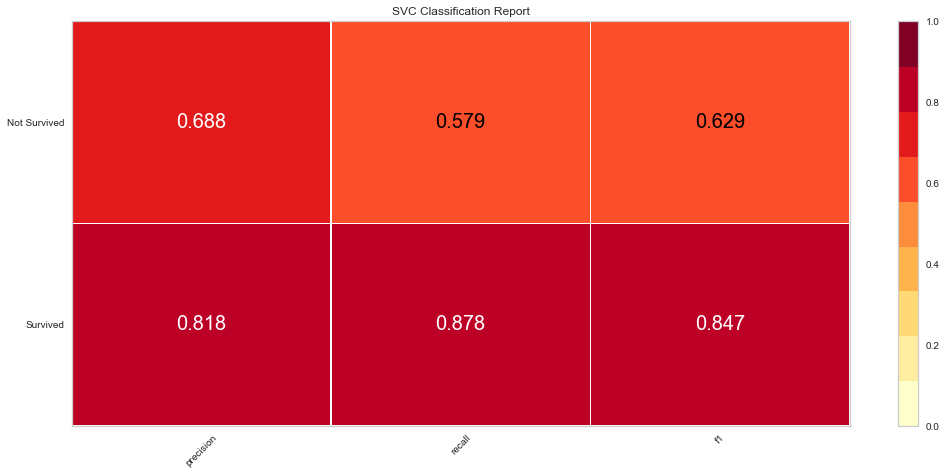
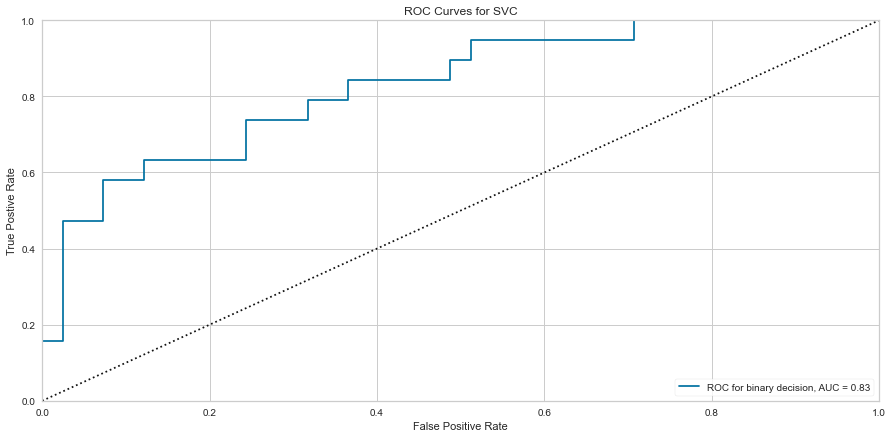
Support vector machine was run using the same parameters. This model had a low number of false negatives at 8 people incorrectly predicted. The F1 scores were higher than the logistic regression model at 0.847 for predicting survival and 0.629 for predicting death. The ROC was slightly better at 0.83. Overall, this appears to be marginally better. Checking feature importance, creatinine, age, cpk, and female gender were all highly important. The one difference is that the presence of anemia and current smoking also appeared to be relatively important in the model.
Random Forest
#Importing Packages
from sklearn.ensemble import RandomForestClassifier
#Resetting Features and Targets
features = df.loc[:, df.columns != 'Event']
target = df['Event']
#Train/Test 80/20 Split
features_train, features_test, target_train, target_test = train_test_split(features, target, test_size = 0.2)
#Creating Object
rfc = RandomForestClassifier(n_estimators = 100, random_state = 1)
rfc.fit(features_train, target_train)
#Visualizing Confusion Matrix, Class Report, and ROC Curve
rfc_cm = ConfusionMatrix(rfc, classes = classes, percent = False)
rfc_cm.fit(features_train, target_train)
rfc_cm.score(features_test, target_test)
rfc_cm.poof()
rfc_class = ClassificationReport(rfc, classes = classes)
rfc_class.fit(features_train, target_train)
rfc_class.score(features_test, target_test)
rfc_class.poof()
rfc_roc = ROCAUC(rfc)
rfc_roc.fit(features_train, target_train)
rfc_roc.score(features_test, target_test)
rfc_roc.poof()
#Checking Feature Importance
labels = list(map(lambda x: x.title(), features))
viz = FeatureImportances(rfc, labels = labels)
viz.fit(features_train, features_test)
viz.show()
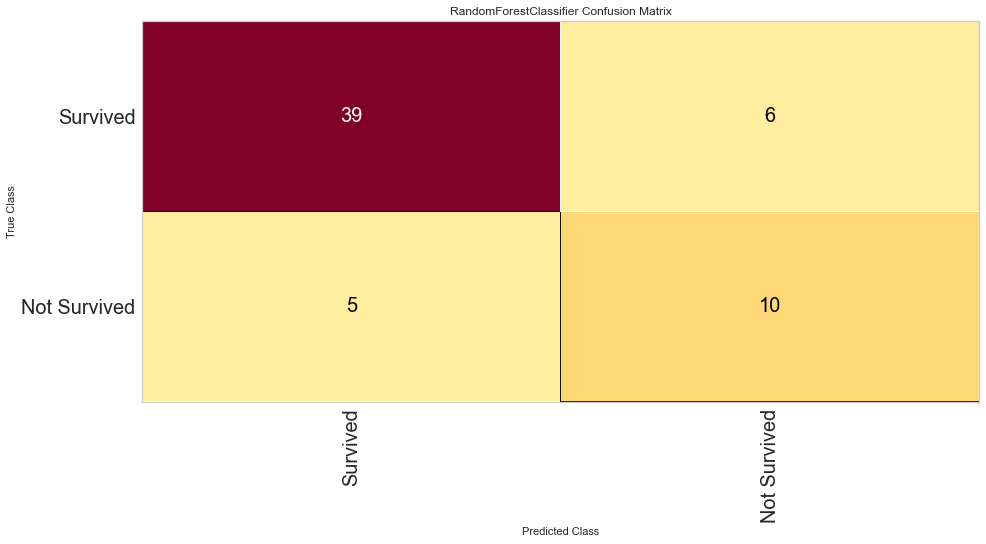
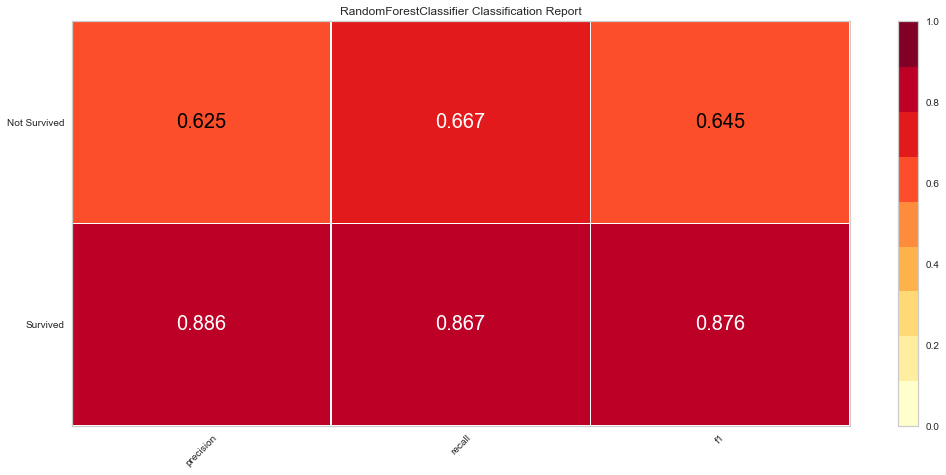
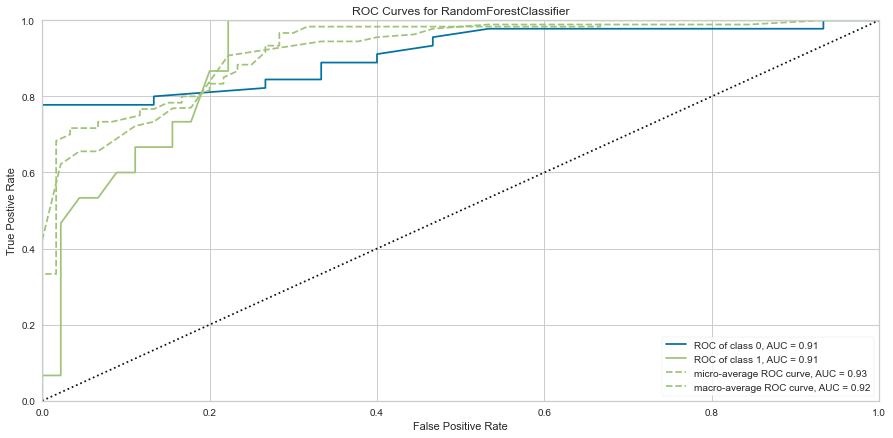
This model performed quite well. It had only 5 false negatives and an F1 score of 0.645 for predicting death, and 0.876 for predicting survival. The ROC was 0.91 for both classes.
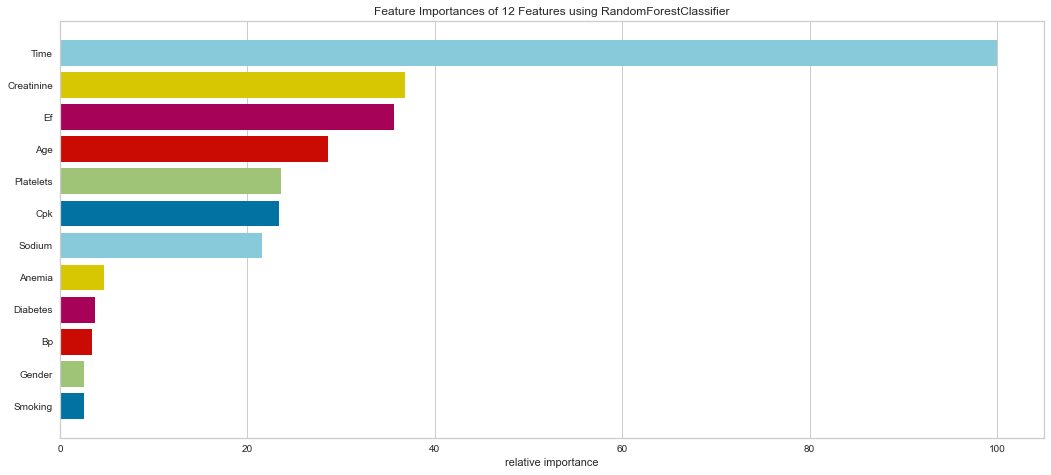
It is interesting that in this model, the ensemble method put a high weight on follow-up time. Creatinine, EF, CPK, Age, Platelets, and Sodium levels were all highly important. Gender was less important in this model. This result is interesting in that EF is directly tied to prognosis in heart failure patients and sodium level can be indicative of fluid balance. Abnormal sodium levels can indicate worsening heart failure symptoms, so this makes medical sense.
XG Boost
#Importing Packages
from xgboost import XGBClassifier
features = pd.get_dummies(features)
target = df['Event']
#Train/Test 80/20 Split
features_train, features_test, target_train, target_test = train_test_split(features, target, test_size = 0.2)
xgb = XGBClassifier(random_state = 1)
xgb.fit(features_train, target_train)
#Visualizing Confusion Matrix, Class Report, and ROC Curve
xgb_cm = ConfusionMatrix(xgb, classes = classes, percent = False)
xgb_cm.fit(features_train, target_train)
xgb_cm.score(features_test, target_test)
xgb_cm.poof()
xgb_class = ClassificationReport(xgb, classes = classes)
xgb_class.fit(features_train, target_train)
xgb_class.score(features_test, target_test)
xgb_class.poof()
xgb_roc = ROCAUC(xgb)
xgb_roc.fit(features_train, target_train)
xgb_roc.score(features_test, target_test)
xgb_roc.poof()
#Checking Feature Importance
labels = list(map(lambda x: x.title(), features))
viz = FeatureImportances(xgb, labels = labels)
viz.fit(features_train, features_test)
viz.show()
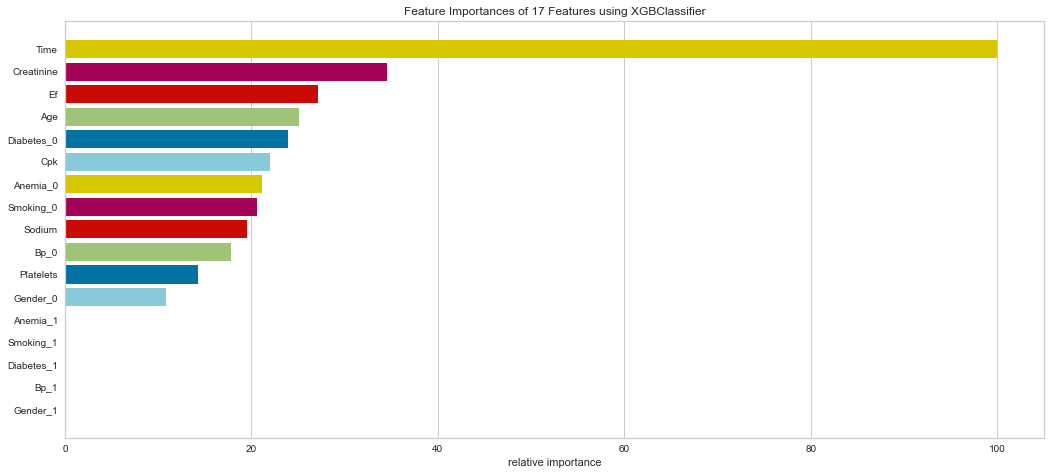
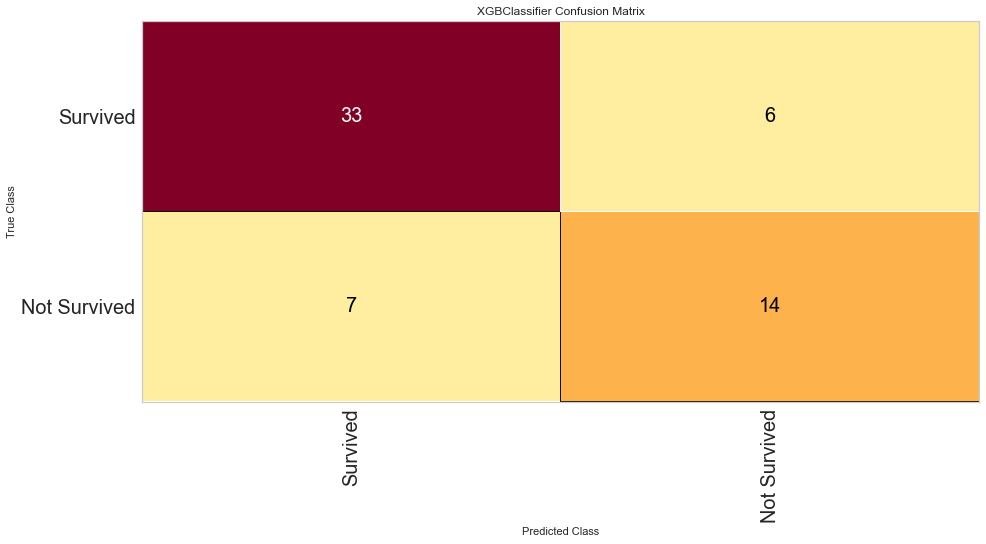
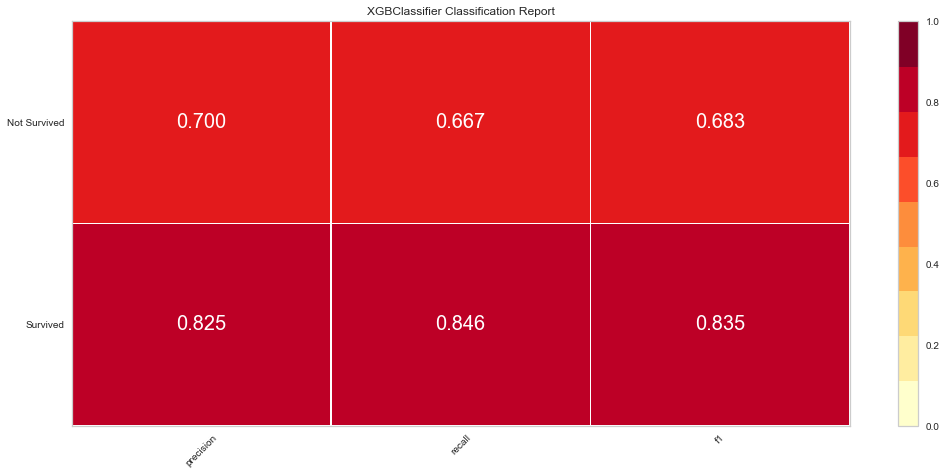
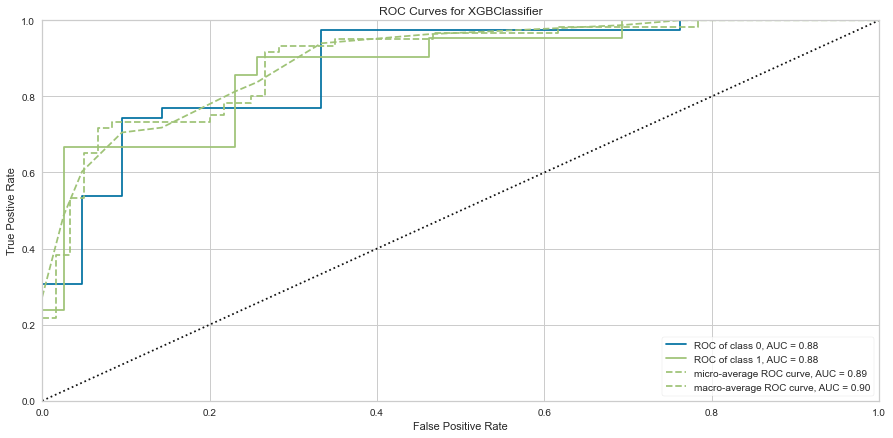
This model also performed quite well. There were only 7 false negatives. The F1 score for predicting death was 0.683 and predicting survival was 0.835. The ROC was 0.88. Feature importance showed a similar result to the Random Forest method showing that time of follow-up, creatinine, EF, female gender, age, and sodium level were all important among several others.
Conclusions
Heart failure is a very deadly disease. There have been significant pharmacologic advancements in recent years which have improved survival. Those with heart failure can have hospital admissions for fluid overload, trouble breathing, and other cardiac events. However, heart failure survival is still dependent upon the severity of the symptoms and other objective measurements as well as early diagnosis and treatment. Therefore, it is timely that we may be able to utilize machine learning algorithms to help better predict death. Perhaps if we can predict a higher risk of death based on severity of various lab measurements and other risk factors, there could be an intensification of therapy and/or aggressive follow-up and monitoring to ensure adequate care and prolonged symptom-free survival.
It is not a significant surprise that the Random Forest and XG Boost models performed the best based on ROC and F1 scores. The Random Forest managed to edge out the XG Boost performance by a small margin. Since both of these are ensemble methods, they have multiple algorithms that are being evaluated and the prediction is then confirmed using a majority vote option. Which model to use is somewhat arbitrary given their largely similar results.
In this population of patients, there were significantly more people alive than dead at the end of the study period. This explains why many of the models predicted more to be alive than dead on a relative basis. The ensemble methods performed the best at this showing the power of these algorithm to be able to predict the harder class (death).
This is the point of this project; we want to primarily identify those at high risk of mortality to either perform some sort of intervention or close monitoring. However, predicting survival can also be beneficial in that if a patient were to be predicted to survive by certain criteria, you could ensure certain factors about their health are optimized and be reassured.
Finally, it is fascinating that the machine learning algorithms all seemed to agree on certain variables that were relatively more important to the prediction. The majority of them noted age, creatinine, CPK, and female gender to have more predictive power. The ensemble methods picked up on more of the traditional variables of sodium, ejection fraction, among others. Many of these variables are already medically validated as related to heart failure prognosis. The machine learning algorithms, at least based on this dataset, agreed with these factors. These factors do differ slightly based on the different algorithms used but many of the algorithms picked out similar important variables.
This dataset is smaller and has a small number of patients. This is partly due to the low numbers of heart failure overall, which limits its predictive power when faced with new data. Much larger datasets would be necessary among a large patient demographic to apply to the general population.
For full code of the project, please refer to my GitHub repository under Applied Data Science.